Antidepressant use and cognitive decline in patients with dementia: a national cohort study – BMC Medicine
Advertisement
BMC Medicine
volume 23, Article number: 82 (2025)
Cite this article
478 AltmetricMetrics detailsDementia is associated with psychiatric symptoms but the effects of antidepressants on cognitive function in dementia are understudied. We aimed to investigate the association between antidepressants and cognitive decline in patients with dementia, and the risk of severe dementia, fractures and death, depending on antidepressant class, drug, and dose.This is a national cohort study. Patients with dementia registered in the Swedish Registry for Cognitive/Dementia Disorders-SveDem from May 1, 2007, until October 16, 2018, with at least one follow-up after dementia diagnosis, and who were new users of antidepressants, were included. Antidepressant use as a time varying exposure defined during the 6 months leading up to dementia diagnosis or each subsequent follow-up. We used linear mixed models to examine the association between antidepressant use and cognitive trajectories assessed by Mini-Mental State Examination (MMSE) scores. We used Cox proportional hazards models to calculate the hazard ratios for severe dementia (MMSE score < 10), fracture, and death. We compared antidepressant classes and drugs, and analyzed dose–response.We included 18740 patients (10 205 women [54.5%]; mean [SD] age, 78.2[7.4] years), of which 4271 (22.8%) received at least one prescription for an antidepressant. During follow-up, a total of 11912 prescriptions for antidepressants were issued, with selective serotonin reuptake inhibitors (SSRI) being the most common (64.8%). Antidepressant use was associated with faster cognitive decline (β (95% CI) = − 0.30(− 0.39, − 0.21) points/year), in particular sertraline (− 0.25(− 0.43, − 0.06) points/year), citalopram (− 0.41(− 0.55, − 0.27) points/year), escitalopram (− 0.76(− 1.09, − 0.44) points/year), and mirtazapine (− 0.19(− 0.34, − 0.04) points/year) compared with non-use. The association was stronger in patients with severe dementia (initial MMSE scores 0–9). Escitalopram showed a greater decline rate than sertraline. Compared with non-use, dose response of SSRIs on greater cognitive decline and higher risks of severe dementia, all-cause mortality, and fracture were observed.In this cohort study, current antidepressant use was associated with faster cognitive decline; furthermore, higher dispensed doses of SSRIs were associated with higher risk for severe dementia, fractures, and all-cause mortality. These findings highlight the significance of careful and regular monitoring to assess the risks and benefits of different antidepressants use in patients with dementia.
Peer Review reports
Antidepressants are widely used in patients with dementia to improve neuropsychiatric symptoms, such as anxiety, depression, aggression, and sleep disorders [1]. Selective serotonin reuptake inhibitors (SSRIs) and serotonin norepinephrine reuptake inhibitors (SNRIs) are considered first-line pharmacotherapy for depression due to fewer side effects compared to other classes of antidepressants. However, older adults with depression receiving SSRIs/SNRIs were associated with an increased risk of dementia compared to psychotherapy [2].
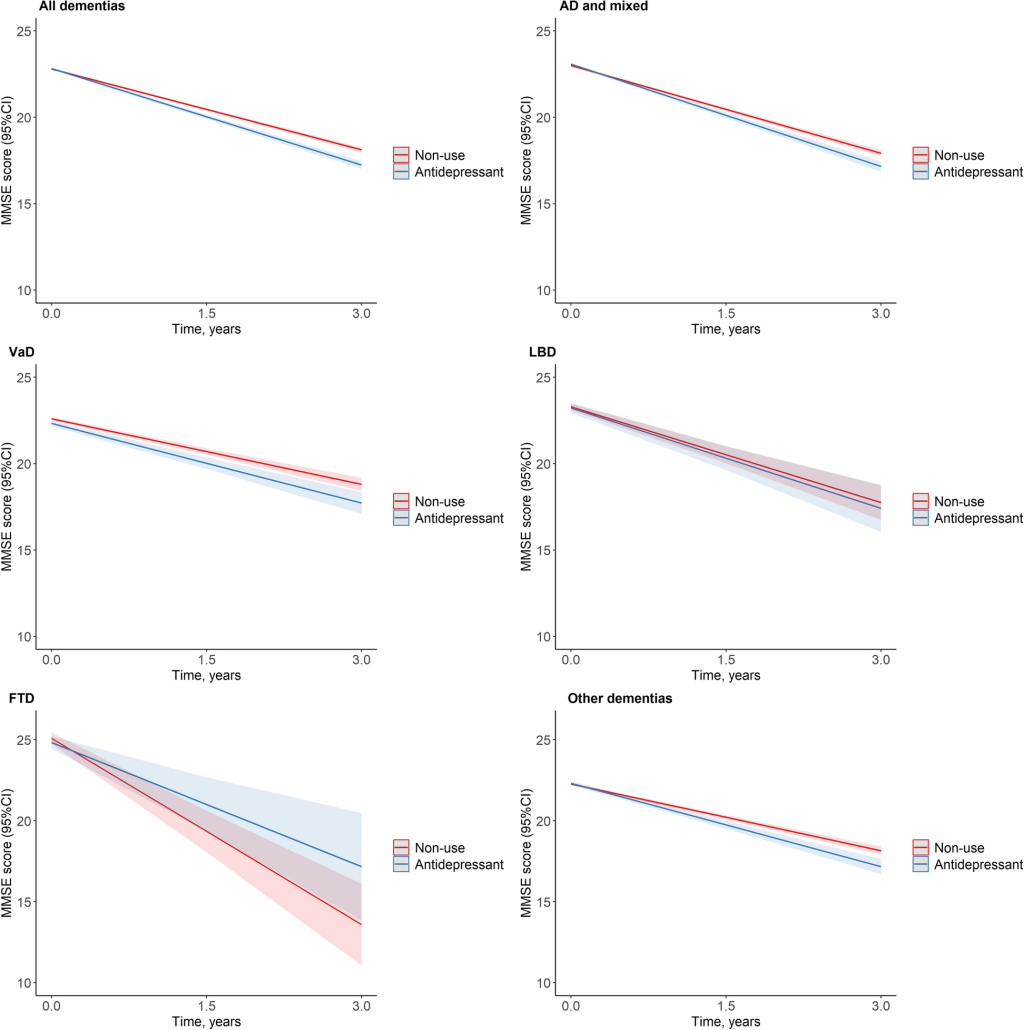
The clinical efficacy of antidepressants on dementia progression is uncertain. Tricyclic antidepressants (TCAs) are anticholinergics and negatively impact cognition [3]. In contrast, a beneficial impact of SSRIs on neurogenesis and pathologic biomarkers, including amyloid burden and tau deposits, has been reported [4, 5], along with evidence suggesting they may delay the progression from mild cognitive impairment (MCI) to Alzheimer’s dementia (AD) [6, 7] among persons with depression. The different cognitive effects of antidepressant classes may be due to the different mechanisms of action, driven by how these drugs proximally act on various neurotransmitters in the brain [3]. Based on the national guidelines for care of depression and anxiety syndrome in Sweden, sertraline and escitalopram form the first-line of therapy for older patients [8]. However, antidepressants do not seem to work as well in people with dementia, and dysfunctions of cognitive control in dementia appears to decrease the effectiveness of some SSRIs [9].Findings from observational studies investigating the impact of antidepressant use on cognitive outcomes are inconclusive. Some longitudinal data observed slower declines in cognition with antidepressant use in patients with AD [10, 11], while most of the cohort studies found no evidence for an association between antidepressant use and post-treatment cognitive decline [12,13,14,15], and negative associations of antidepressant use with subsequent cognitive impairment has been reported [16, 17]. Previous analyses were limited to the period before dementia diagnosis [15], a single population, such as patients with depression but not in patients with dementia [12, 14, 16], a short-term follow-up 11 [13], and reporting the effect of antidepressants on cognition as a secondary outcome [17]. There is a gap in understanding how different antidepressant classes, specific drugs, and doses affect the progression of cognitive decline in patients with dementia. Moreover, existing studies have not thoroughly explored how individual factors, such as age, sex, and dementia severity, may modify the association between antidepressant use and cognitive outcomes.Some antidepressants have anticholinergic activities which could contribute to worse cognition, and potentially, falls and mortality, particularly in dementia types with cholinergic deficit such as AD and dementia with Lewy bodies (DLB) [18,19,20]. Moreover, previous studies were conducted mainly in patients with AD; findings related to other dementias, such as vascular dementia (VaD) [21], frontotemporal dementia (FTD) [22], DLB [23], and Parkinson’s disease dementia (PDD) are scarce. Long-term follow-up studies are difficult due to high attrition rates and loss of follow-up [24]. Currently, direct comparisons of different individual drugs on cognitive decline in patients with dementia are lacking.This study examines the long-term effect of antidepressants on cognitive decline, fractures, and mortality in patients with dementia. It aims to address the knowledge gap by providing a comprehensive analysis of how different antidepressant classes, drugs, and doses impact dementia progression, and whether factors like dementia subtypes, severity, and medications modify these effects. The findings may inform clinical care and contribute to future research, providing insights for primary care practitioners and specialists involved in dementia healthcare.Based on nationwide Swedish registers, we conducted a population-based cohort study between May 1, 2007, and October 16, 2018. Using the Swedish Registry for Cognitive/Dementia Disorders (SveDem), we identified patients with incident diagnosed dementia. SveDem is a quality registry established in 2007 aiming to register and follow-up all patients with incident dementia in Sweden. SveDem includes patients with incident dementia diagnosis from either primary care or specialist memory clinics and contains information on demographics, diagnostic process, and cognitive and mortality outcomes. For this study, we used the type of dementia, cognitive evaluation by MMSE, coresident status, and type of diagnostic unit from SveDem [25]. The National Patient Register contains nationwide records on inpatient care since 1987 and more than 80% of specialized (hospital-based) outpatient care since 2001 [26]. The Swedish Prescribed Drug Register provides complete data on dispensation of prescription medications from all pharmacies since July 2005 [27]. The Cause of Death Registry contains data on overall and specific mortality and dates of death [28]. The Swedish unique personal identity number was used to identify patients across sources and to merge data.The study population included patients with incident dementia registered in SveDem between May 1, 2007, and October 16, 2018. We defined index date as the date of the dementia diagnosis in SveDem. We excluded patients if any of the following applied: missing information on MMSE score at baseline; a record of antidepressant dispensation prior to the 6-month period before the date of dementia diagnosis or no follow-ups. To permit comparisons between drugs, we also excluded patients who received prescriptions for different antidepressants within a class or antidepressants from different classes in the same 6-month period. Additional file 1: Figure S1 presents a flowchart for the selection of participants.Dementia disorders are clinically diagnosed and recorded according to the International Classification of Diseases, Tenth Revision (ICD-10) codes [29], with the McKeith criteria [30] used for DLB, the Lund-Manchester criteria [31] for FTD, and the Movement Disorder Society Task Force criteria [32] for PDD, respectively (Additional file 2: Table S1). Dementia was defined at the time of the establishment of the dementia diagnosis, coded as AD, mixed dementia, VaD, DLB, FTD, PDD, and other dementias, which included unspecified dementia and other dementia types not classified above. DLB and PDD share pathological and clinical characteristics, are considered part of a continuum within the spectrum of LBD [33, 34], and were therefore merged for this study as LBDs.We treated antidepressant use as a time varying exposure and defined it as a dispensation of medication during the 6 months leading up to the dementia diagnosis or each subsequent follow-up date through the Prescribed Drug Register by ATC codes (Additional file 2: Table S2). This is followed by grouping of antidepressant drugs into five classes according to the mode of action: SSRIs, SNRIs, TCAs, and other antidepressants.We extracted information on the dose of each dispensation of antidepressants within the 6-month period preceding each SveDem entry date or each subsequent follow-up date. Cumulative doses dispensed during these time periods were expressed as number of defined daily doses (DDD) in each package or dispensation. The DDD for each medication is defined by the World Health Organization [35] and was used to allow dose comparisons between different medications. When multiple dispensations were used, their DDD were added [36].The main outcome for this study was cognitive decline, defined as MMSE score change over the years. Information of baseline and follow-up MMSE scores were collected from SveDem. The secondary outcomes included severe dementia, fracture, and death. Severe dementia was specifically defined as MMSE score < 10 during follow-up [37]. Information of death from all causes was extracted from the Cause of Death Registry based on ICD-10 codes. Data on fractures, defined as any fractures occurring at skeletal sites during follow-up, were extracted from the National Patient Register and Cause of Death Registry by using the ICD-10 codes (Additional file 2: Table S3). Patients were observed from index date through October 16, 2018, for any secondary outcomes.We defined covariates at the index date, including age, sex, coresident status, type of diagnostic unit, and calendar year of diagnosis. We used ICD-10 codes to identify common and major physical disorders diagnosed within 3 years before the date of dementia diagnosis from the National Patient Register (Additional file 2: Table S3). We used the Charlson Comorbidity Index score [38] (CCIs) to assess medical comorbidities, using a weighted sum of diagnosed chronic disorders [39] but excluding dementia. In addition, we also included depression and fracture diagnosed within 3 years before the date of dementia diagnosis (Additional file 2: Table S3).Data on medications were ascertained by ATC codes and defined as the presence of filled pharmacy prescriptions within the 6 months prior to and at the date of dementia diagnosis, including angiotensin-converting enzyme inhibitors/angiotensin receptor blockers, β-blocking agents, calcium channel blockers, nonsteroidal anti-inflammatory drugs, diuretics, lipid-modifying agents, antiplatelets, antipsychotics, anxiolytics, and hypnotics (Additional file 2: Table S4). Anti-dementia medications (i.e., cholinesterase inhibitors [ChEIs] and memantine) use was defined as a dispensation of medication during the 6 months after dementia diagnosis (Additional file 2: Table S4).We used linear mixed models to examine the associations between the use of antidepressants and cognitive decline (MMSE score change) over the years. We treated antidepressant use as a time varying exposure to account for patients stopping treatment and changing between treatments during follow-up. We considered patients to be exposed to treatment if no gaps of more than 90 days existed between the end of one prescription and the start of the next. Follow-up time was treated as a continuous measure defined as years since first cognitive assessment. The model included antidepressant use and follow-up time and an interaction between drug use and time. Following our previous work in SveDem [36], a linear trend over time was assumed and the model allowed for a random intercept and random slope for each patient. We also included the inverse probability of censoring weighting considering the potential effects of dropout or to the presence of a competing risk before the end of follow-up such as death [40].In addition to examining any dementias, we separately examined the effects for different subtypes of dementia (AD and mixed, VaD, LBD, FTD, and other dementias). The beta coefficients (β) and 95% confidence intervals (CIs) were obtained from adjusted models including age, sex, calendar year of dementia diagnosis, the type of dementia, MMSE score at diagnosis, coresident status, type of diagnostic unit, depression, fracture, CCIs, and medications. For patients diagnosed with AD, mixed dementia, and LBD, we further adjusted for ChEIs and memantine.The analysis was initially conducted for any antidepressant, followed by each class of antidepressants (SSRIs, SNRIs, TCAs, and other antidepressants) compared with no current treatment. We compared use of individual antidepressant drugs with no current treatment when numbers were sufficient. In addition, different antidepressant classes and individual drugs were directly compared. We investigated the impact of antidepressant dosage by examining it as a continuous variable and categorizing it into three groups within each class (≤ 0.5 DDD, > 0.5/ ≤ 1.0 DDD, > 1.0DDD). Given that 94.8% of patients prescribed TCAs were using a low dose (≤ 0.5 DDD) (Additional file 2: Table S5), the analysis comparing SSRIs and TCAs, specifically citalopram (SSRI) and amitriptyline (TCA), was performed within the low-dose group (≤ 0.5 DDD).We did subgroup analysis to explore the potential effects of age (median < 78, ≥ 78 years), sex (male/female), coresident status (cohabiting or living alone), type of diagnostic unit (specialist care or primary care), living in nursing home, calendar year of diagnosis (2007–2012, 2013–2018), baseline MMSE score (0–9, 10–19, 20–24, 25–30) and current use of antipsychotics, anxiolytics and hypnotics, on the association between antidepressant use and cognitive decline. Interaction tests between these factors and antidepressant use were conducted separately to assess possible modifying effects. For patients diagnosed with AD and mixed dementia, and LBD, we also conducted stratified analysis by current use of ChEIs and memantine.We estimated crude incidence rates per 1000 person-years for fracture and all-cause death in all patients at the end of follow-up, and severe dementia in patients who had baseline MMSE score > 10. We used time-dependent Cox proportional hazards models to estimate the associations between time-varying antidepressants and each outcome and calculated the hazard ratios (HRs) with 95% confidence intervals (CIs). We used time since cohort entry as the underlying timescale. Considering the high mortality of patients with dementia after diagnosis, we applied a competing risk model for outcomes of severe dementia and fracture.Since depression itself has been linked with dementia and cognitive impairment [41, 42], we did a sensitivity analysis among patients without depression to reduce the indication bias. Furthermore, to avoid floor effects, we did a sensitivity analysis among patients with MMSE ≥ 10 and without depression, excluding patients with baseline severe dementia.Statistical analyses were conducted with SAS version 9.4 (SAS Institute Inc, Cary, NC) and R 4.2.1, with statistical tests using a 2-tailed P < 0.05 as the level of statistical significance.In total, 18,740 patients were included in this cohort study, 10,205 (54.5%) were women. The mean (SD) age and MMSE score at baseline were 78.2 (7.4) years and 22.1 (4.3), respectively (Additional file 2: Table S6). The total number of person-years of follow-up was 80,737, with a mean (SD) of 4.3 (2.2) years per patient.During follow-up, a total of 11,912 prescriptions for antidepressants were issued, 4271 (22.8%) patients received at least one prescription for an antidepressant. SSRIs were the most commonly prescribed class, accounting for 64.8%, followed by TCAs (2.2%), SNRIs (2.0%), and the group of other antidepressants (31.0%) (Additional file 1: Figure S2 and Additional file 2: Table S5). The six most commonly prescribed antidepressant drugs comprised 99.0% (n = 11 788) of all prescriptions, including citalopram (SSRI), mirtazapine (other), sertraline (SSRI), escitalopram (SSRI), amitriptyline (TCA), and venlafaxine (SNRI), were analyzed separately in some analysis.Compared with non-use, antidepressant use was associated with faster cognitive decline (β = − 0.30 points/year; 95% CI, − 0.39 to − 0.21) during follow-up (Fig. 1 and Table 1). The results were largely similar for AD and mixed dementia (β = − 0.28 points/year; 95% CI, − 0.40 to − 0.16), VaD (β = − 0.27 points/year; 95% CI, − 0.52 to − 0.02), and other dementias (β = − 0.34 points/year; 95% CI, − 0.52 to − 0.16), except LBD and FTD (Fig. 1 and Table 1).Estimated MMSE trajectories between use of antidepressants and non-use by dementia subtypesa. Abbreviations: SveDem, the Swedish Registry for Cognitive/Dementia Disorders; CIs, confidence intervals; MMSE, Mini-Mental State Examination; AD, Alzheimer’s disease; Mixed, mixed dementia; VaD, vascular dementia; LBD, Parkinson’s disease with dementia and dementia with Lewy bodies; FTD, frontotemporal dementia.a, Estimated MMSE trajectories from mixed model, adjusted for age, sex, calendar year of diagnosis, the type of dementia, MMSE score at diagnosis, coresident status, care unit, depression, fracture, Charlson Comorbidity Index score , medications (angiotensin-converting enzyme inhibitors (ACEIs)/angiotensin receptor blockers (ARBs), β-blocking agents, calcium channel blockers, nonsteroidal anti-inflammatory drugs, diuretics, lipid-modifying agents, antiplatelets, antipsychotics, anxiolytics, and hypnotics). For patients with AD and mixed dementia and LBD, models further adjusted for cholinesterase inhibitors and memantineWe also observed similar significant results for antidepressant classes for SSRIs (β = − 0.39 points/year; 95% CI, − 0.50 to − 0.28) and other antidepressants (β = − 0.20 points/year; 95% CI, − 0.35 to − 0.05) and individual antidepressant drugs for sertraline (SSRI) (β = − 0.25 points/year; 95% CI, − 0.43 to − 0.06), citalopram (SSRI) (β = − 0.41 points/year; 95% CI, − 0.55 to − 0.27), escitalopram (SSRI) (β = − 0.76 points/year; 95% CI, − 1.09 to − 0.44), and mirtazapine (other) (β = − 0.19 points/year; 95% CI, − 0.34 to − 0.04) (Fig. 2 and Table 2).Estimated MMSE trajectories between use of antidepressants and non-use by antidepressant class and individual drugsa. Abbreviations: SveDem, the Swedish Registry for Cognitive/Dementia Disorders; CIs, confidence intervals; MMSE, Mini-Mental State Examination; SSRIs, selective serotonin reuptake inhibitors; SNRIs, serotonin and norepinephrine reuptake inhibitors; TCAs, Tricyclic antidepressants; Others, other antidepressants. a, Estimated MMSE trajectories from mixed model, adjusted for age, sex, calendar year of diagnosis, the type of dementia, MMSE score at diagnosis, coresident status, care unit, depression, fracture, Charlson Comorbidity Index score, medications (angiotensin-converting enzyme inhibitors (ACEIs)/angiotensin receptor blockers (ARBs), β-blocking agents, calcium channel blockers, nonsteroidal anti-inflammatory drugs, diuretics, lipid-modifying agents, antiplatelets, antipsychotics, anxiolytics, and hypnotics)In addition, compared with sertraline (SSRI), escitalopram (SSRI) (β = − 0.51 points/year; 95% CI, − 0.89 to − 0.12) presented faster cognitive decline, while citalopram (SSRI) (β = 0.28 points/year; 95% CI, 0.17 to 0.39) showed slower cognitive decline (Fig. 3 and Table 2).Estimated MMSE trajectories across antidepressant classes and individual drugsa. Abbreviations: SveDem, the Swedish Registry for Cognitive/Dementia Disorders; CIs, confidence intervals; MMSE, Mini-Mental State Examination; SSRIs, selective serotonin reuptake inhibitors; SNRIs, serotonin and norepinephrine reuptake inhibitors; TCAs, Tricyclic antidepressants; Others, other antidepressants. a, Estimated MMSE trajectories from mixed model, adjusted for age, sex, calendar year of diagnosis, the type of dementia, MMSE score at diagnosis, coresident status, care unit, depression, fracture, Charlson Comorbidity Index score, medications (angiotensin-converting enzyme inhibitors (ACEIs)/angiotensin receptor blockers (ARBs), β-blocking agents, calcium channel blockers, nonsteroidal anti-inflammatory drugs, diuretics, lipid-modifying agents, antiplatelets, antipsychotics, anxiolytics, and hypnotics)Higher dispensed doses of antidepressants, specifically for SSRIs and the group of other antidepressants were associated with faster cognitive decline during follow-up (Table 3 and Additional file 1: Figure S3). Similar results were observed in sensitivity analysis among patients diagnosed with AD and mixed dementia, patients without depression or patients with baseline MMSE ≥ 10 and without depression (Additional file 1: Figure S3 and Additional file 2: Table S7-S10).
Subgroup analysis of the associations between antidepressants and cognitive decline is shown in Table 4. Compared with patients who were women, had higher MMSE score at baseline, using anxiolytics and hypnotics, the effect size of cognitive decline was greater in those who were men, had lower MMSE score, not using anxiolytics or hypnotics. Modifying effects of sex and use of anxiolytics on the association between antidepressant use and cognitive decline were observed (P for interaction < 0.05). A slower cognitive decline was observed in younger (< 78 years) patients with FTD (β = 1.61 points/year; 95% CI, 0.05 to 3.17). Patients with the lowest initial MMSE scores (0–9) exhibited the greatest subsequent cognitive decline (β = − 1.51 points/year; 95% CI, − 2.82 to − 0.20). Furthermore, the results were similar between users and non-users of ChEIs; among patients not using memantine, compared with non-use, antidepressant use showed faster cognitive decline for patients diagnosed with AD and mixed dementia (β = − 0.30 points/year; 95% CI, − 0.45 to − 0.15), and for LBD (β = − 0.85 points/year; 95% CI, − 1.64 to − 0.06) (Additional file 1: Figure S4 and Additional file 2: Table S11). There were no significant differences between subgroups of coresident status, type of diagnostic unit, living in nursing home, calendar year of dementia diagnosis, and current use of antipsychotics on cognitive decline.
Compared with non-use, antidepressant use was associated with higher risk of all-cause mortality (HR = 1.07; 95% CI, 1.01 to 1.13) and fracture (HR = 1.18; 95% CI, 1.10 to 1.26) (Additional file 2: Table S12-S14). Higher dispensed dose (> 1.0 DDD) of SSRIs were associated with increased risk of severe dementia (HR = 1.35; 95% CI, 1.02 to 1.80), all-cause mortality (HR = 1.18; 95% CI, 1.07 to 1.31), and fracture (HR = 1.25; 95% CI, 1.10 to 1.43), compared with non-use (Additional file 2: Table S12-S14). Consistent results were observed in patients with AD and mixed dementia (Additional file 2: Table S15).In this nationwide cohort study, we found that the current use of antidepressants was associated with faster cognitive decline in patients with dementia compared with non-use, and this association was driven mainly by patients with severe dementia. Higher dispensed doses of SSRIs were associated with more cognitive decline during follow-up, and higher risk of severe dementia, fracture, and all-cause mortality.Previous studies of antidepressant use and cognitive decline in people with dementia have shown mixed findings. Most clinical trials reporting the effect of antidepressants on neuropsychiatric symptoms and cognition, did so as a secondary or safety outcome [43, 44]. In the majority of the cases reported, antidepressants had the same effect on cognition as placebo [44,45,46,47], but some reported a significant decline on the MMSE scores in antidepressant users [43, 48]. Many of the clinical trials were too small to provide precise estimates of the moderate benefits on cognition that might realistically be expected [49]. A recently conducted RCT reported worsening of cognition in patients with AD who used citalopram over 9 weeks [43]. In contrast, other RCTs in AD indicated that another two SSRIs, sertraline and escitalopram, had no effect on cognitive function [49, 50]. Individual antidepressants even within same class cannot be considered identical drugs. Evidence has shown some differences regarding the speed of onset of response and adverse events among individual SSRIs [51]. Recent findings demonstrated that specifically sertraline, escitalopram, and mirtazapine had relatively higher responses and lower dropout profile compared to other antidepressants [52]. These differences may influence medication choice for a given patient and may show varied effect on dementia progression. More studies are needed to explore the underlying mechanisms, optimal timing for intervention, and the types of patients who would benefit the most from these specific medications.Our study showed significantly faster cognitive decline in patients with SSRIs (i.e., citalopram, sertraline, and escitalopram) compared to non-use. However, the magnitude of the effect of citalopram (0.41 points/year), sertraline (0.25 points/year), and escitalopram (0.76 points/year) appears to be lower than the minimum clinically significant change in MMSE score of 1–3 points [53]. A meta-analysis that included 15 RCTs involving a total of 1616 patients with AD found that second-generation antidepressants had no effect on global cognition measured by MMSE, and this remained in subgroup analyses of duration of medication, drug classes, combination with anti-dementia medication, various NPS, and degree of AD [47]. However, results from meta-analyses may be biased without adjustment for the clinical status of patients such as chronic physical disease and are not quantitatively assessed since most of the trials included used flexible doses of antidepressants. Sertraline and escitalopram are first hand choices for depression among older individuals in Sweden [8]. However, antidepressants do not seem to work as well in patients with dementia, possibly because “depression in dementia is a different illness” than depression in people with intact cognition [54]. Cognitive control dysfunction in dementia appears to decrease the effectiveness of some SSRIs [9]. In our study, we found SSRIs were associated with a small negative impact on cognitive functioning, but its clinical significance is uncertain.Evidence regarding the long-term effect of antidepressants on cognitive decline in VaD is lacking. In previous open-label studies in patients with VaD [21], MMSE score increased significantly in the fluoxetine (SSRI) group but not in the control group. Another study conducted in patients with vascular cognitive impairment without dementia [55] found that, compared with controls, fluoxetine (SSRI) was associated with better performance on Ten Point Clock drawing test, indicating better cognitive functioning and greater ability to understand spatial relationships, plan, and execute tasks, but no significant differences in change of Alzheimer’s Disease Assessment Scale cognitive subscale score. In this study, we found that antidepressant use was associated with a significant decline in cognition in patients with VaD compared to non-use. Furthermore, we also observed a slower cognitive decline in younger (< 78 years) patients with FTD. In line with our observation, Laura et al. [56] found that citalopram can partially restore the dysfunctional prefrontal cortical systems by increasing serotonergic neurotransmission in FTD. Future long-term studies are warranted to validate our findings.Some antidepressants, such as TCAs, are anticholinergic and combining these with acetylcholinesterase inhibitors is counterintuitive due to their conflicting mechanisms of action [57]. Our study showed the association between antidepressant use and cognitive decline was not modified by use of ChEIs but was worse in non-users of memantine. In a RCT (n = 95) among older adults with major depression and memory complains, a combination of memantine and escitalopram significantly improved delayed recall and executive functioning at 12 months [58]. However, the differences in specific antidepressants or anti-dementia drugs, sample size, and cognitive function at baseline might be the main reason related to the heterogeneity between studies.Population-based cohort studies have found that antidepressant use was related to no or lower risks of all-cause mortality in patients with dementia [59, 60], but increased risk of fracture [61, 62]. In our study, we found that SSRIs were associated with increased risks of all-cause mortality and fracture compared with no current treatment. Thus, careful and regular monitoring is needed to assess the risks and benefits of different antidepressants and decrease the risk of adverse events.This study has several strengths, including a large nationally representative cohort of individuals with dementia, long follow-up assessments, and a range of different types of dementia. In addition, demographic characteristics, medical disorders, and characteristics related to dementia were also explored. To our knowledge, this is the first systematic assessment of the long-term effects of commonly used antidepressants on cognition in patients with dementia. Our medication exposure was time-dependent, taking into account the change in prescribing patterns that occur after dementia diagnosis and thus more accurately reflective of medication use at the time of event. Furthermore, we had detailed information on prescriptions for antidepressants throughout the follow-up period, so we could do comprehensive analyses investigating effects of individual drugs and dose.This study has limitations. The main concern is indication bias, which occurs when patients are prescribed drugs for a condition that is itself associated with the outcome of interest. Depression has been linked with dementia and cognitive impairment in normal people with depression [41, 42], which means that the associations with antidepressants may be due to depression for which it was prescribed rather than to the drug itself. To reduce this bias, we repeated and restricted our main analysis to include only patients without depression and found consistent results. In addition, in this study only patients who were new users of antidepressants were included, previous users of antidepressants with depression were not included. However, the clinical diagnosis of depression was obtained through specialized in- and out-patient care, which primarily represents more severe manifestations: less severe depression is generally managed through primary care and would have been missed. And there is an overlap in symptoms between depression and dementia, making diagnosing depression particularly challenging in these cases. Furthermore, we did not have information on the severity of depression and actual intake of antidepressants, only dispensation. Residual confounding due to lack of diagnosis of depression in dementia would thus reduce the differences between antidepressants users and non-users since more individuals are likely to end up erroneously in the group of non-users. However, many patients with dementia seem to have received antidepressant medications for other neuropsychiatric symptoms, as the sensitivity analyses among non-depressed patients did not change the results. But the direct comparisons among treated groups exhibit reduced susceptibility to confounding by indication or factors influencing treatment prescription. Second, although direct comparisons between antidepressant classes or drugs could to some extent reduce the influence of neuropsychiatric symptoms, they may still be influenced by channeling bias. This bias can occur when distinct antidepressant drugs with similar indications are prescribed based on varying patient characteristics [52]. Third, the severity of dementia could independently contribute to cognitive decline, making it difficult to definitively attribute the observed effects solely to antidepressant use. However, we observed antidepressant use was associated with faster cognitive decline in patients with different MMSE scores at dementia diagnosis, though the effect size of cognitive decline was greater in patients with lower MMSE score. Future research is needed to further elucidate the complex interplay between antidepressant use, dementia severity, and cognitive decline. Fourth, SveDem is a real-world database, which suffers from significant patient loss to follow-up. In this study, we calculated and adjusted the inverse probability of censoring weighting to address the issue of selective dropouts. Furthermore, the national coverage of SveDem for new dementia cases is not absolute, it covers 100% of memory clinics and 75% of primary care units, and almost one-third of all expected new dementia cases in Sweden [63, 64]. Thus, the generalizability of our findings to other populations remains to be studied. However, the dementia diagnostic workup follows standard clinical practice, and few patients have a changed dementia diagnosis at follow-up, which suggests adequate diagnostic accuracy [65]. Lastly, some of the analyses were imprecisely estimated due to the small number of patients with some individual antidepressants and in stratified analysis.In this cohort study, use of antidepressants was associated with faster cognitive decline in patients with dementia, in particular SSRIs (i.e., citalopram, sertraline and escitalopram) and mirtazapine. These effects appeared to be more pronounced in patients with more severe dementia. Compared with sertraline, escitalopram presented faster cognitive decline, while citalopram was linked to a slower cognitive decline. Additionally, higher dispensed doses of SSRIs were associated with greater cognitive decline, as well as increased risks of severe dementia, all-cause mortality, and fracture. Our study cannot distinguish whether these findings are due to the antidepressants or the underlying psychiatric indication.Following the Swedish and EU legislation, the data are not available for public access. In order to obtain the data from Swedish registries, researches must apply to the steering committees of the registries as well as relevant government authorities, after obtaining the ethical approval.Alzheimer’s dementiaCharlson Comorbidity Index scoreCholinesterase inhibitorsConfidence intervalsDefined daily dosesDementias with Lewy bodiesFrontotemporal dementiaHazard ratiosInternational Classification of Diseases, Tenth RevisionMild cognitive impairmentMini-Mental State ExaminationParkinson’s disease dementiaRandomized controlled trialsSerotonin norepinephrine reuptake inhibitorsSelective serotonin reuptake inhibitorsSwedish Registry for Cognitive/Dementia DisordersTricyclic antidepressantsVascular dementiaTampi RR, Jeste DV. Dementia Is More Than Memory Loss: Neuropsychiatric Symptoms of Dementia and Their Nonpharmacological and Pharmacological Management. Am J Psychiatry. 2022;179(8):528–43.PubMed
Google Scholar
Wang GHM, Chen WH, Chang SH, Zhang TX, Shao H, Guo JC, Lo-Ciganic WH. Association between first-line antidepressant use and risk of dementia in older adults: a retrospective cohort study. Bmc Geriatrics. 2023;23(1).Blumberg MJ, Vaccarino SR, McInerney SJ. Procognitive Effects of Antidepressants and Other Therapeutic Agents in Major Depressive Disorder: A Systematic Review. J Clin Psychiatry. 2020;81(4).Cirrito JR, Disabato BM, Restivo JL, Verges DK, Goebel WD, Sathyan A, et al. Serotonin signaling is associated with lower amyloid-beta levels and plaques in transgenic mice and humans. Proc Natl Acad Sci U S A. 2011;108(36):14968–73.CAS
PubMed
PubMed Central
Google Scholar
Sheline YI, West T, Yarasheski K, Swarm R, Jasielec MS, Fisher JR, et al. An antidepressant decreases CSF Abeta production in healthy individuals and in transgenic AD mice. Sci Transl Med. 2014;6(236):236re4.PubMed
PubMed Central
Google Scholar
Pelton GH, Harper OL, Roose SP, Marder K, D’Antonio K, Devanand DP. Combined treatment with memantine/es-citalopram for older depressed patients with cognitive impairment: a pilot study. Int J Geriatr Psychiatry. 2016;31(6):648–55.PubMed
Google Scholar
Bartels C, Wagner M, Wolfsgruber S, Ehrenreich H, Schneider A. Alzheimer’s Disease Neuroimaging I. Impact of SSRI Therapy on Risk of Conversion From Mild Cognitive Impairment to Alzheimer’s Dementia in Individuals With Previous Depression. Am J Psychiatry. 2018;175(3):232–41.PubMed
Google Scholar
committee RSsm. KLOKA LISTAN 2024. Stockholm, Sweden: Stockholm County Council; 2024. Available from: https://klokalistan.se/download/18.2eb60b5b18d2a87a7321b413/1706013022004/Kloka_Listan_2024_webb_20240123.pdf. Cited 2024 03 March.Rubin R. Exploring the Relationship Between Depression and Dementia. JAMA. 2018;320(10):961–2.PubMed
Google Scholar
Dutcher SK, Rattinger GB, Langenberg P, Chhabra PT, Liu X, Rosenberg PB, et al. Effect of medications on physical function and cognition in nursing home residents with dementia. J Am Geriatr Soc. 2014;62(6):1046–55.PubMed
PubMed Central
Google Scholar
Rozzini L, Chilovi BV, Conti M, Bertoletti E, Zanetti M, Trabucchi M, Padovani A. Efficacy of SSRIs on cognition of Alzheimer’s disease patients treated with cholinesterase inhibitors. Int Psychogeriatr. 2010;22(1):114–9.PubMed
Google Scholar
Carriere I, Norton J, Farre A, Wyart M, Tzourio C, Noize P, et al. Antidepressant use and cognitive decline in community-dwelling elderly people - The Three-City Cohort. BMC Med. 2017;15(1):81.PubMed
PubMed Central
Google Scholar
Caballero J, Hitchcock M, Beversdorf D, Scharre D, Nahata M. Long-term effects of antidepressants on cognition in patients with Alzheimer’s disease. J Clin Pharm Ther. 2006;31(6):593–8.CAS
PubMed
Google Scholar
Saczynski JS, Rosen AB, McCammon RJ, Zivin K, Andrade SE, Langa KM, et al. Antidepressant Use and Cognitive Decline: The Health and Retirement Study. Am J Med. 2015;128(7):739–46.CAS
PubMed
PubMed Central
Google Scholar
Vom Hofe I, Stricker BH, Vernooij MW, Ikram MK, Ikram MA, Wolters FJ. Antidepressant use in relation to dementia risk, cognitive decline, and brain atrophy. Alzheimers Dement. 2024;20(5):3378–87.
Google Scholar
Goveas JS, Hogan PE, Kotchen JM, Smoller JW, Denburg NL, Manson JE, et al. Depressive symptoms, antidepressant use, and future cognitive health in postmenopausal women: the Women’s Health Initiative Memory Study. Int Psychogeriatr. 2012;24(8):1252–64.PubMed
PubMed Central
Google Scholar
Rosenberg PB, Mielke MM, Han D, Leoutsakos JS, Lyketsos CG, Rabins PV, et al. The association of psychotropic medication use with the cognitive, functional, and neuropsychiatric trajectory of Alzheimer’s disease. Int J Geriatr Psychiatry. 2012;27(12):1248–57.PubMed
PubMed Central
Google Scholar
Garcia-Ptacek S, Kramberger MG. Parkinson Disease and Dementia. J Geriatr Psych Neur. 2016;29(5):261–70.
Google Scholar
Bohnen NI, Kaufer DI, Ivanco LS, Lopresti B, Koeppe RA, Davis JG, et al. Cortical cholinergic function is more severely affected in parkinsonian dementia than in Alzheimer disease - An in vivo positron emission tomographic study. Arch Neurol-Chicago. 2003;60(12):1745–8.PubMed
Google Scholar
Tan ECK, Eriksdotter M, Garcia-Ptacek S, Fastbom J, Johnell K. Anticholinergic Burden and Risk of Stroke and Death in People with Different Types of Dementia. Journal of Alzheimers Disease. 2018;65(2):589–96.CAS
Google Scholar
Liu X, Zhang J, Sun D, Fan Y, Zhou H, Fu B. Effects of fluoxetine on brain-derived neurotrophic factor serum concentration and cognition in patients with vascular dementia. Clin Interv Aging. 2014;9:411–8.PubMed
PubMed Central
Google Scholar
Deakin JB, Rahman S, Nestor PJ, Hodges JR, Sahakian BJ. Paroxetine does not improve symptoms and impairs cognition in frontotemporal dementia: a double-blind randomized controlled trial. Psychopharmacology. 2004;172(4):400–8.CAS
PubMed
Google Scholar
Culo S, Mulsant BH, Rosen J, Mazumdar S, Blakesley RE, Houck PR, Pollock BG. Treating neuropsychiatric symptoms in dementia with Lewy bodies: a randomized controlled-trial. Alzheimer Dis Assoc Disord. 2010;24(4):360–4.PubMed
Google Scholar
Courtney C, Farrell D, Gray R, Hills R, Lynch L, Sellwood E, et al. Long-term donepezil treatment in 565 patients with Alzheimer’s disease (AD2000): randomised double-blind trial. Lancet. 2004;363(9427):2105–15.CAS
PubMed
Google Scholar
Religa D, Fereshtehnejad SM, Cermakova P, Edlund AK, Garcia-Ptacek S, Granqvist N, et al. SveDem, the Swedish Dementia Registry - a tool for improving the quality of diagnostics, treatment and care of dementia patients in clinical practice. PLoS ONE. 2015;10(2): e0116538.PubMed
PubMed Central
Google Scholar
Ludvigsson JF, Andersson E, Ekbom A, Feychting M, Kim JL, Reuterwall C, et al. External review and validation of the Swedish national inpatient register. BMC Public Health. 2011;11:450.PubMed
PubMed Central
Google Scholar
Wettermark B, Hammar N, Fored CM, Leimanis A, Otterblad Olausson P, Bergman U, et al. The new Swedish Prescribed Drug Register–opportunities for pharmacoepidemiological research and experience from the first six months. Pharmacoepidemiol Drug Saf. 2007;16(7):726–35.PubMed
Google Scholar
(Socialstyrelsen). NBoHaW. Dödsorsaksregistret Sweden: National Board of Health and Welfare (Socialstyrelsen); 2023. Available from: https://www.socialstyrelsen.se/statistik-och-data/register/dodsorsaksregistret/.Organization WH. The ICD-10 classification of mental and behavioural disorders, clinical descriptions and diagnostic guidelines. Geneva: World Health Organization; 1992.
Google Scholar
Castagnini A, Berrios GE. Acute and transient psychotic disorders (ICD-10 F23): a review from a European perspective. Eur Arch Psychiatry Clin Neurosci. 2009;259(8):433–43.PubMed
Google Scholar
Association AP. Diagnostic and statistical manual of mental disorders (DSM-IV). 4th ed. Washington, DC: American Psychiatric Association; 1994.
Google Scholar
Kendell RE. Clinical validity. Psychol Med. 1989;19(1):45–55.CAS
PubMed
Google Scholar
Fereshtehnejad SM, Religa D, Westman E, Aarsland D, Lokk J, Eriksdotter M. Demography, diagnostics, and medication in dementia with Lewy bodies and Parkinson’s disease with dementia: data from the Swedish Dementia Quality Registry (SveDem). Neuropsychiatr Dis Treat. 2013;9:927–35.PubMed
PubMed Central
Google Scholar
Ballard C, Garcia-Ptacek S, van Steenoven I, Aarsland D. 241Spectrum of Lewy body dementias: relationship of Parkinson’s disease dementia to dementia with Lewy bodies. In: Emre M, editor. Cognitive Impairment and Dementia in Parkinson's Disease: Oxford University Press; 2015. p. 0.Organization WH. Defined Daily Dose: Essential Medicines and Health Products: ATC/DDD Toolkit: World Health Organization. Available from: https://www.who.int/toolkits/atc-ddd-toolkit/about-ddd.Xu H, Garcia-Ptacek S, Jonsson L, Wimo A, Nordstrom P, Eriksdotter M. Long-term Effects of Cholinesterase Inhibitors on Cognitive Decline and Mortality. Neurology. 2021;96(17):e2220–30.CAS
PubMed
PubMed Central
Google Scholar
Dementia: Assessment, management and support for people living with dementia and their carers. National Institute for Health and Care Excellence: Guidelines. London 2018.Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–83.CAS
PubMed
Google Scholar
Quan H, Sundararajan V, Halfon P, Fong A, Burnand B, Luthi JC, et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med Care. 2005;43(11):1130–9.PubMed
Google Scholar
Handels R, Jonsson L, Garcia-Ptacek S, Eriksdotter M, Wimo A. Controlling for selective dropout in longitudinal dementia data: Application to the SveDem registry. Alzheimers Dement. 2020;16(5):789–96.PubMed
Google Scholar
Byers AL, Yaffe K. Depression and risk of developing dementia. Nat Rev Neurol. 2011;7(6):323–31.CAS
PubMed
PubMed Central
Google Scholar
Diniz BS, Butters MA, Albert SM, Dew MA, Reynolds CF 3rd. Late-life depression and risk of vascular dementia and Alzheimer’s disease: systematic review and meta-analysis of community-based cohort studies. Br J Psychiatry. 2013;202(5):329–35.PubMed
PubMed Central
Google Scholar
Porsteinsson AP, Drye LT, Pollock BG, Devanand DP, Frangakis C, Ismail Z, et al. Effect of citalopram on agitation in Alzheimer disease: the CitAD randomized clinical trial. JAMA. 2014;311(7):682–91.CAS
PubMed
PubMed Central
Google Scholar
Dudas R, Malouf R, McCleery J, Dening T. Antidepressants for treating depression in dementia. Cochrane Database Syst Rev. 2018;8(8):CD003944.PubMed
Google Scholar
Maier F, Spottke A, Bach JP, Bartels C, Buerger K, Dodel R, et al. Bupropion for the Treatment of Apathy in Alzheimer Disease: A Randomized Clinical Trial. JAMA Netw Open. 2020;3(5): e206027.PubMed
PubMed Central
Google Scholar
Mowla A, Mosavinasab M, Haghshenas H, Borhani HA. Does serotonin augmentation have any effect on cognition and activities of daily living in Alzheimer’s dementia? A double-blind, placebo-controlled clinical trial. J Clin Psychopharmacol. 2007;27(5):484–7.CAS
PubMed
Google Scholar
Qin M, Wu J, Zhou Q, Liang Z, Su Y. Global cognitive effects of second-generation antidepressants in patients with Alzheimer’s disease: A systematic review and meta-analysis of randomized controlled trials. J Psychiatr Res. 2022;155:371–9.PubMed
Google Scholar
Teri L, Logsdon RG, Peskind E, Raskind M, Weiner MF, Tractenberg RE, et al. Treatment of agitation in AD: a randomized, placebo-controlled clinical trial. Neurology. 2000;55(9):1271–8.CAS
PubMed
Google Scholar
Choe YM, Kim KW, Jhoo JH, Ryu SH, Seo EH, Sohn BK, et al. Multicenter, randomized, placebo-controlled, double-blind clinical trial of escitalopram on the progression-delaying effects in Alzheimer’s disease. Int J Geriatr Psychiatry. 2016;31(7):731–9.PubMed
Google Scholar
Munro CA, Longmire CF, Drye LT, Martin BK, Frangakis CE, Meinert CL, et al. Cognitive outcomes after sertaline treatment in patients with depression of Alzheimer disease. Am J Geriatr Psychiatry. 2012;20(12):1036–44.PubMed
PubMed Central
Google Scholar
Gartlehner G, Gaynes BN, Hansen RA, Thieda P, DeVeaugh-Geiss A, Krebs EE, et al. Comparative benefits and harms of second-generation antidepressants: background paper for the American College of Physicians. Ann Intern Med. 2008;149(10):734–50.PubMed
Google Scholar
Cipriani A, Furukawa TA, Salanti G, Chaimani A, Atkinson LZ, Ogawa Y, et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis. Lancet. 2018;391(10128):1357–66.CAS
PubMed
PubMed Central
Google Scholar
Andrews JS, Desai U, Kirson NY, Zichlin ML, Ball DE, Matthews BR. Disease severity and minimal clinically important differences in clinical outcome assessments for Alzheimer’s disease clinical trials. Alzheimers Dement (N Y). 2019;5:354–63.PubMed
Google Scholar
Alexopoulos GS, Manning K, Kanellopoulos D, McGovern A, Seirup JK, Banerjee S, Gunning F. Cognitive control, reward-related decision making and outcomes of late-life depression treated with an antidepressant. Psychol Med. 2015;45(14):3111–20.CAS
PubMed
PubMed Central
Google Scholar
Zhang L, Liu X, Li T, Xu B, Fu B. Fluoxetine May Enhance VEGF, BDNF and Cognition in Patients with Vascular Cognitive Impairment No Dementia: An Open-Label Randomized Clinical Study. Neuropsychiatr Dis Treat. 2021;17:3819–25.CAS
PubMed
PubMed Central
Google Scholar
Hughes LE, Rittman T, Regenthal R, Robbins TW, Rowe JB. Improving response inhibition systems in frontotemporal dementia with citalopram. Brain. 2015;138(Pt 7):1961–75.PubMed
PubMed Central
Google Scholar
Johnell K, Fastbom J. Concurrent use of anticholinergic drugs and cholinesterase inhibitors: register-based study of over 700,000 elderly patients. Drugs Aging. 2008;25(10):871–7.CAS
PubMed
Google Scholar
Lavretsky H, Laird KT, Krause-Sorio B, Heimberg BF, Yeargin J, Grzenda A, et al. A Randomized Double-Blind Placebo-Controlled Trial of Combined Escitalopram and Memantine for Older Adults With Major Depression and Subjective Memory Complaints. Am J Geriat Psychiat. 2020;28(2):178–90.
Google Scholar
Su JA, Chang CC, Wang HM, Chen KJ, Yang YH, Lin CY. Antidepressant treatment and mortality risk in patients with dementia and depression: a nationwide population cohort study in Taiwan. Ther Adv Chronic Dis. 2019;10:2040622319853719.PubMed
PubMed Central
Google Scholar
Enache D, Fereshtehnejad SM, Kareholt I, Cermakova P, Garcia-Ptacek S, Johnell K, et al. Antidepressants and mortality risk in a dementia cohort: data from SveDem, the Swedish Dementia Registry. Acta Psychiatr Scand. 2016;134(5):430–40.CAS
PubMed
Google Scholar
Zakarias JK, Norgaard A, Jensen-Dahm C, Gasse C, Laursen TM, Palm H, et al. Risk of hospitalization and hip fracture associated with psychotropic polypharmacy in patients with dementia: A nationwide register-based study. Int J Geriatr Psychiatry. 2021;36(11):1691–8.PubMed
Google Scholar
Bakken MS, Engeland A, Engesaeter LB, Ranhoff AH, Hunskaar S, Ruths S. Increased risk of hip fracture among older people using antidepressant drugs: data from the Norwegian Prescription Database and the Norwegian Hip Fracture Registry. Age Ageing. 2013;42(4):514–20.PubMed
Google Scholar
SveDem. Svenska Demensregistret Årsrapport 2022 Sweden2022. Available from: https://www.ucr.uu.se/svedem/om-svedem/arsrapporter/svedemarsrapport-2022/viewdocument/1077. Cited 2023 Oct 18.Mo M, Zacarias-Pons L, Hoang MT, Mostafaei S, Jurado PG, Stark I, et al. Psychiatric Disorders Before and After Dementia Diagnosis. JAMA Netw Open. 2023;6(10): e2338080.PubMed
PubMed Central
Google Scholar
Garcia-Ptacek S, Farahmand B, Kareholt I, Religa D, Cuadrado ML, Eriksdotter M. Mortality risk after dementia diagnosis by dementia type and underlying factors: a cohort of 15,209 patients based on the Swedish Dementia Registry. J Alzheimers Dis. 2014;41(2):467–77.PubMed
Google Scholar
Download referencesThe authors are grateful to SveDem (www.svedem.se) for providing data for this study. We thank all patients, caregivers, reporting units and coordinators in SveDem as well as SveDem steering committee. SveDem is supported financially by the Swedish Associations of Local Authorities and Regions.Open access funding provided by Karolinska Institute. This project is supported by the Swedish Research Council (Garcia-Ptacek 2022–01425, Hong 2022–01428), StratNeuro start-up grant (the Strategic Research Area Neuroscience-Karolinska Institutet, Umeå University and KTH, Hong), Karolinska Institutet research foundations (Garcia-Ptacek), Emil and Wera Cornell Foundation (Garcia-Ptacek), Johanniterorden I Sverige/Swedish Order of St. John, Stiftelsen för Sigurd och Elsa Goljes Minne (Garcia-Ptacek), the Center for Innovative Medicine Foundation (Hong, CIMED, FoUI-963369), Åke Wibergs stiftelse (Hong M22-0170), U&L Angeby stiftelse (Hong 2022–02882), Karolinska Institutet Research Foundation (Minjia 2024–02322), Swedish Research Council for Health, Working Life and Welfare (Forte, Minjia 2024–01295).Division of Clinical Geriatrics, Department of Neurobiology, Care Sciences and Society, Karolinska Institutet, Blickagången 16, Stockholm, 14152, SwedenMinjia Mo, Tamar Abzhandadze, Minh Tuan Hoang, Simona Sacuiu, Pol Grau Jurado, Luana Naia, Silvia Maioli, Hong Xu, Maria Eriksdotter & Sara Garcia-PtacekDepartment of Occupational Therapy and Physiotherapy, Sahlgrenska University Hospital, Rehabiliteringsmedicin, Vita Stråket 12, Vån 4, Gothenburg, 41345, SwedenTamar AbzhandadzeDepartment of Medical Epidemiology and Biostatistics, Karolinska Institutet, Nobels Väg 12a, Stockholm, 17165, SwedenMinh Tuan HoangDepartment of Neuropsychiatry, Sahlgrenska University Hospital Mölndal, Region Västra Götaland, Sweden, Wallinsgatan 6, Mölndal, 43141, SwedenSimona SacuiuDepartment of Psychiatry and Neurochemistry, Institute of Neuroscience and Physiology, Neuropsychiatric Epidemiology (EPINEP), Sahlgrenska Academy, University of Gothenburg, Medicinaregatan 3, Göteborg, 413 90, SwedenSimona SacuiuTheme Inflammation and Aging, Medical Unit Aging, Karolinska University Hospital, Karolinska Vägen 37A, Stockholm, 171 64, SwedenSimona Sacuiu, Maria Eriksdotter & Sara Garcia-PtacekDepartment of Clinical Neurosciences, Karolinska Institutet, Nobels Väg 9, Stockholm, D3, 17165, SwedenJoana B. PereiraDepartment of Laboratory Medicine, Team Neurovascular Biology and Health, Clinical Immunology, Karolinska Institutet, H5 Laboratoriemedicin, H5 Klin Immunologi Bergman, Huddinge, 14152, SwedenJulianna KeleYou can also search for this author in
PubMed Google ScholarYou can also search for this author in
PubMed Google ScholarYou can also search for this author in
PubMed Google ScholarYou can also search for this author in
PubMed Google ScholarYou can also search for this author in
PubMed Google ScholarYou can also search for this author in
PubMed Google ScholarYou can also search for this author in
PubMed Google ScholarYou can also search for this author in
PubMed Google ScholarYou can also search for this author in
PubMed Google ScholarYou can also search for this author in
PubMed Google ScholarYou can also search for this author in
PubMed Google ScholarYou can also search for this author in
PubMed Google ScholarMJM contributed to study design, analysis, interpretation of data, draft and revise the manuscript. SGP contributed to study design, acquisition of data, revise the manuscript and interpretation of data. SS contributed to study design, acquisition and interpretation of data, and revise the manuscript. ME contributed to interpretation of data and revise the manuscript. TA, MTH, PGJ, JBP, LN, JK, SM and HX contributed to interpretation of data and revise the manuscript. All authors critically revised the manuscript and approved the final version of the manuscript.Correspondence to
Minjia Mo or Sara Garcia-Ptacek.The requirement of written consent for this study was waived due to the register data being pseudonymized before delivery to our research group. The regional ethics committee in Stockholm approved the study (dnr 2017/501–31; 2017/942–32), which complies with the Declaration of Helsinki 31. Participants and caretakers are informed verbally about SveDem and could decline participation.Not applicable.The authors declare no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations. Additional file 1: Figure S1. Flowchart of study patients with dementia. Figure S2. Distribution of dosages of antidepressants by antidepressant class. Figure S3. Estimated MMSE trajectories between use of antidepressants and non-use by dose in patients from SveDem, 2007–2018 a . Figure S4. Estimated MMSE trajectories between use of antidepressants and non-use stratified by dementia medications in patients from SveDem, 2007–2018a. Additional file 2: Table S1. ICD-10 codes for dementia and subtypes. Table S2. ATC codes for antidepressants. Table S3. ICD-10 codes for comorbidities. Table S4. ATC codes for medications. Table S5. Defined daily doses (DDD) by antidepressant classes. Values are numbers of prescriptions (column percentages). Table S6. Baseline characteristics of dementia patients. Table S7. Associations of antidepressants dose with cognitive decline by antidepressant class in patients from SveDem, 2007–2018. Table S8. Associations of antidepressants with cognitive decline by antidepressant class in patients diagnosed with AD and mixed dementia from SveDem. Table S9. Associations between antidepressants and cognitive decline in patients without depression, 2007–2018. Table S10. Associations between antidepressants and cognitive decline in patients with baseline MMSE ≥ 10 and without depression, 2007–2018. Table S11. Stratified analysis of associations between antidepressants and cognitive decline by dementia medications in patients with AD and mixed dementia and LBD from SveDem, 2007–2018. Table S12. Hazard ratios for adverse outcomes by antidepressant class and dose in patients from SveDem, 2007–2018. Table S13. Incidence Rate for adverse outcomes by antidepressant class in patients from SveDem, 2007–2018. Table S14. Incidence rate for adverse outcomes by antidepressant class and dose in patients from SveDem, 2007–2018. Table S15. Incidence Rate and hazard ratios for adverse outcomes by antidepressant class and dementia subtypes in patients from SveDem, 2007–2018.Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.Reprints and permissionsMo, M., Abzhandadze, T., Hoang, M.T. et al. Antidepressant use and cognitive decline in patients with dementia: a national cohort study.
BMC Med 23, 82 (2025). https://doi.org/10.1186/s12916-025-03851-3Download citationReceived: 05 July 2024Accepted: 08 January 2025Published: 25 February 2025DOI: https://doi.org/10.1186/s12916-025-03851-3Anyone you share the following link with will be able to read this content:Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
CollectionAdvertisementISSN: 1741-7015
By using this website, you agree to our
Terms and Conditions,
Your US state privacy rights,
Privacy
statement and
Cookies policy.
Your privacy choices/Manage cookies we use in the preference centre.
© 2025 BioMed Central Ltd unless otherwise stated. Part of
Springer Nature.
Source: https://bmcmedicine.biomedcentral.com/articles/10.1186/s12916-025-03851-3